Mastering MIPS Quality Measures: An In-Depth Look
For healthcare providers, mastering the Merit-based Incentive Payment System (MIPS) Quality category is not merely a regulatory requirement—it's a vital pathway to demonstrating value, optimizing revenue, and ensuring high-quality patient care. As a key part of your total MIPS score, understanding and effectively reporting Quality Measures is crucial. This comprehensive guide simplifies the complexity, offering clear insights and actionable strategies to help you navigate, select, and successfully report MIPS Quality Measures.
What Exactly Are MIPS Quality Measures?
MIPS Quality Measures are specific actions or outcomes related to patient care that CMS uses to assess the quality of services provided by MIPS-eligible clinicians and groups. They are standardized metrics designed to evaluate how effectively providers deliver care across areas such as preventive care, chronic disease management, patient safety, and patient experience.
CMS maintains a detailed list of approved Quality Measures each year. The measures cover a broad range of clinical topics and are developed by various organizations, including medical societies, quality improvement groups, and the Centers for Medicare & Medicaid Services (CMS) itself.
Where Can MIPS Participants Access the List of MIPS Quality Measures?
The primary source for the complete list of MIPS Quality Measures is the CMS Quality Payment Program website. CMS publishes the official MIPS Quality Measures specifications, including detailed information on each measure's denominator, numerator, exclusions, and reporting requirements.
You can usually find the list by navigating to the QPP website and looking for resources related to the current performance year. The measures are typically available in downloadable formats, such as specification documents or spreadsheets, which include the full details.

(A screenshot containing "MIPS Quality Measures." The file is available for download here - https://qpp.cms.gov/resources/document/270ad8af-591f-4e4b-86b1-9c387be4880b)
Understanding Specialty Measure Sets and Their Role in Categorizing MIPS Quality Measures
Specialty Measure Sets are tailored lists of MIPS Quality Measures relevant to specific medical specialties. CMS develops these sets to help clinicians in fields like Cardiology, Dermatology, or Family Medicine identify measures that align with their practice and patient population.
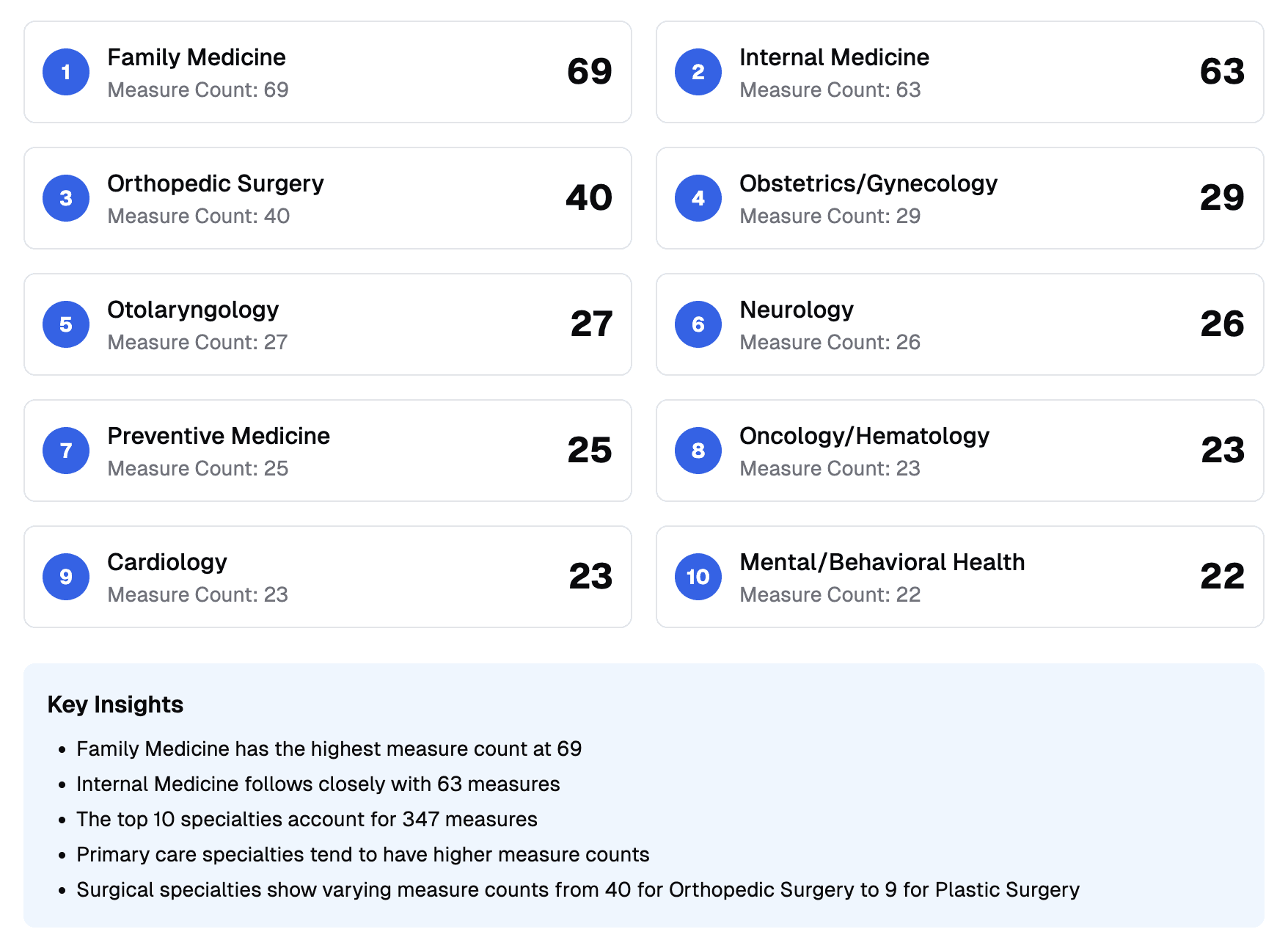
These sets organize the broader list of MIPS Quality Measures by specialty, such as Oncology or Orthopedics. While clinicians are not required to report only from their specialty set, these sets serve as a useful starting point for selecting relevant measures. They simplify the process by presenting a focused list of options. Note that some specialty sets may include more measures than others, reflecting the range of quality metrics in that field.
While specialty measure sets are helpful, your best measure selection might include options outside your set. You are not limited to reporting only from your specialty set, and measures from other areas may better fit your patient population or clinical workflows. Reviewing the complete list of available measures, beyond your specialty set, is recommended to find those where your practice can perform best.
Measure Count by Specialty Measure Set
Exploring the Various Submission Methods for MIPS Quality Measures
CMS offers several options for reporting Quality Measure data, providing flexibility for practices of different sizes and types. The primary submission methods include:
EHR (Electronic Health Record): If your certified EHR technology supports electronic Clinical Quality Measures (eCQMs), you can generate and submit data directly from your EHR. This method relies on structured data mapped to specific measure criteria.
Qualified Registry: Approved third-party organizations collect and submit MIPS data on your behalf. Registries often support a wider range of measures, including MIPS CQMs, which may not be available as eCQMs in your EHR. They can pull data from various sources, like EHRs and practice management systems.
Qualified Clinical Data Registry (QCDR): Similar to registries but focused on specific specialties or conditions. QCDRs report MIPS measures and custom measures approved by CMS for their focus area.
Claims: Small practices (15 or fewer clinicians) can report measures on Medicare Part B claims using CPT II codes or G-codes. This method is limited in measure options and scoring potential due to less detailed data.
CMS Web Interface: Used by large groups and Accountable Care Organizations (ACOs) that registered for it, this method involves reporting specific measures on a sample of Medicare patients. It is being phased out.
CAHPS for MIPS: A survey option for groups of 2+ clinicians to report patient experience measures.
Choosing the right submission method impacts which measures you can report and how you collect data. It depends on factors like practice size, EHR capabilities, and desired analytics support. Some methods, like Qualified Registries and QCDRs, support more measures, including specialty-specific ones, offering better performance potential. CMS allows multiple submission methods and uses the one that results in the highest Quality score.
Understanding Collection Types and Their Impact on Data
While submission methods refer to how you send data to CMS (EHR, Registry, etc.), collection types are the technical standards and data formats required for a measure. They define the rules for the data itself, tied to the submission method.
Each submission method uses one or more collection types:
EHR Submission: Uses eCQMs, requiring structured data in your EHR, like QRDA files.
Registry Submission: Uses MIPS CQMs, which can pull data from a broader range of sources, offering flexibility.
Claims Submission: Relies on claims collection types, using CPT II or G-codes in billing data.
The collection type dictates what data in your systems can be used. For example, an eCQM might need data from a specific EHR field, while a registry CQM can use different fields or integrated systems. Understanding collection types is key to capturing data accurately.
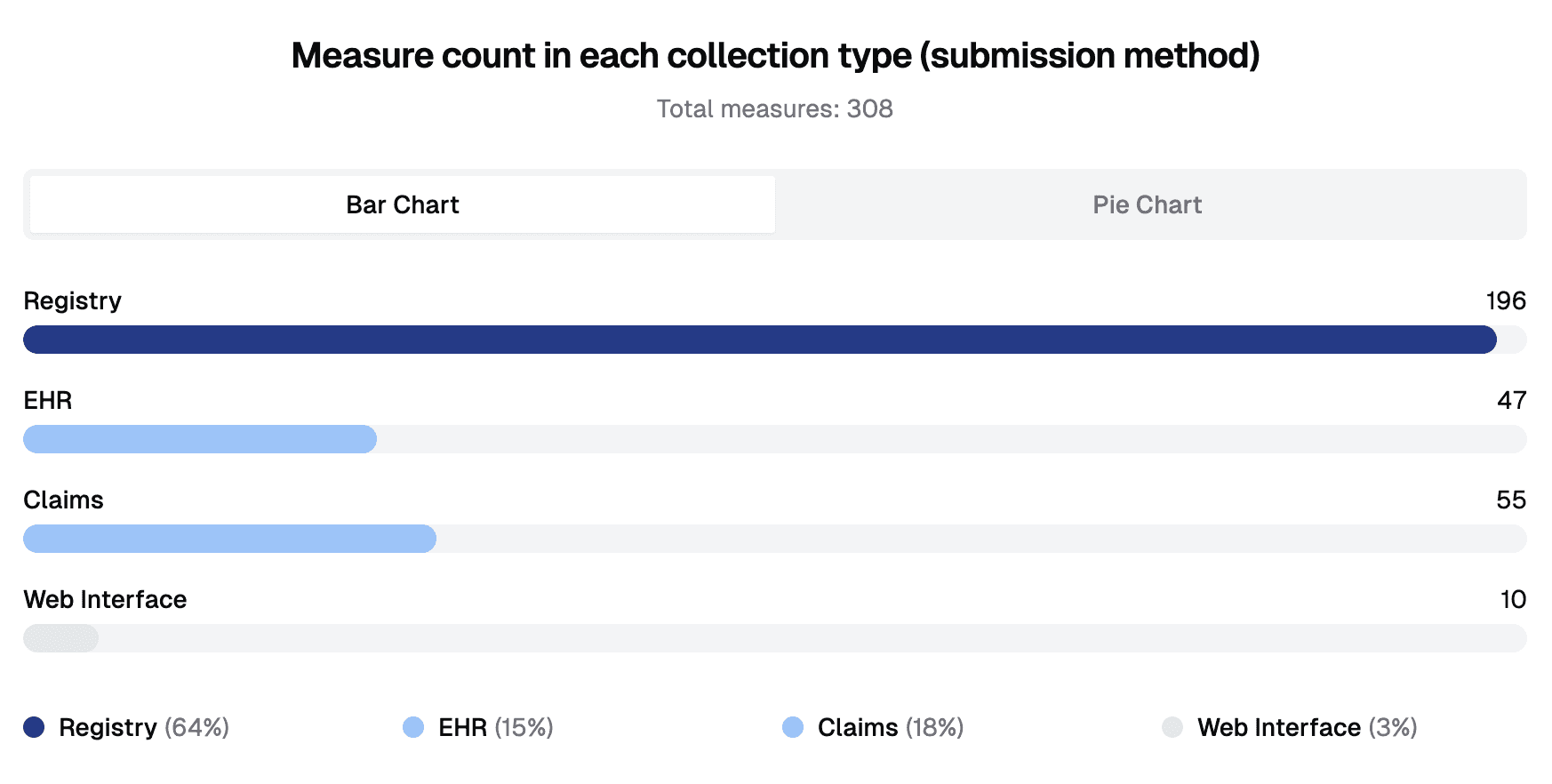
(Measure count in each collection type)
How Are Denominators Determined for MIPS Quality Measures?
The denominator for a MIPS Quality Measure represents the eligible patient population or care instances included in the measure’s calculation. The measure’s specifications outline the denominator criteria, defining the initial pool for the numerator.
Denominator criteria typically narrow the eligible group with factors like:
Age: E.g., “Patients aged 18 years and older.”
Demographics: E.g., “Female patients aged 65+.”
Timeframe/Encounter: E.g., “Patients aged 6 months+ seen between October 1 and March 31.”
Clinical Conditions: E.g., “Patients aged 18-75 with diabetes.”
Multiple Factors: E.g., “Patients 18+ with coronary artery disease and diabetes or a BMI outside normal range.”
Procedures: E.g., “Reports for procedures using fluoroscopy documenting radiation exposure.”
Treatments/Events: E.g., “Patients with cancer receiving chemotherapy or radiation.”
Calculating the denominator accurately means identifying all encounters meeting these criteria. Broad criteria create larger denominators; narrow ones reduce them. You need at least 20 cases to be scored against the benchmark.
How Are Numerators Determined for MIPS Quality Measures?
The numerator is the subset of the denominator where the desired clinical action or outcome occurred, showing your quality performance. The measure’s specifications define the numerator criteria, like an intervention performed or outcome achieved.
For example, in a diabetes measure, the denominator might be “Patients 18-75 with diabetes,” and the numerator is “Patients who had an A1c test.” Calculating the numerator involves tracking which denominator cases met the criteria, requiring clear documentation.
Timing depends on the measure’s case unit:
Patient/Period Units: The action can occur anytime in the period (often a year), allowing flexibility.
Encounter/Procedure Units: The action must happen during or soon after the event (e.g., within 7 days of discharge).
Denominator exclusions (e.g., medical contraindications) and exceptions (e.g., patient refusal) adjust counts. Accurately tracking these ensures correct performance rates.
How Benchmarks Inform Your Performance Score in MIPS Quality Measures
Benchmarks are critical for scoring MIPS Quality Measures. CMS compares your performance rate to historical data from other MIPS participants who reported the same measure and collection type. Benchmarks are specific to each measure and collection type, divided into deciles.
Your performance rate earns 1-10 points based on the decile it falls into:
3-10 points: For meeting or exceeding the 3rd decile.
1-2 points: For lower performance but meeting data completeness and case minimum.
0 points: For missing data completeness or benchmarks.
High benchmarks mean a measure is widely achieved, requiring top performance for high points. Lower benchmarks suggest a tougher measure, where modest results can score well. Understanding benchmarks helps set realistic goals.
For example:
Measure A: 3rd decile is 92%, 10th is 100%. A 95% rate might earn 5-7 points; 99% could hit 9-10.
Measure B: 3rd decile is 25%, 10th is 80%. A 40% rate might earn 5-6 points; 75% could hit 9-10.
Benchmarks reflect how you compare to peers, not a perfect standard.
Additional Factors CMS Uses to Score Your MIPS Quality Performance
Beyond benchmarks, CMS considers:
Data Completeness: Report 75% of eligible cases to earn more than 1-2 points.
Case Minimum: 20+ cases per measure for full scoring.
Topped-Out Measures: High-performing measures may cap at 7 points.
Measure Type: Outcome and high-priority measures (e.g., patient safety) earn bonuses.
Extra Measures: Reporting beyond six measures boosts your score, up to 100 points.
Bonus Points: Earned for electronic reporting or high-priority measures, with caps.
Your Quality score combines achievement points (from benchmarks and rules) and bonuses, capped at 100 points, before weighting in your MIPS score.
Understanding the Reporting Burden Associated with Different MIPS Quality Measures
The “burden” of a measure refers to the effort, resources, and workflow changes needed to collect and report data. Burden varies by:
Data Access: Measures needing data from multiple systems or manual abstraction are harder.
Workflow: Measures requiring new documentation steps add work.
Documentation: Strict requirements for specific notes or codes increase effort.
Patient Volume: Measures with many eligible patients mean more tracking.
Complexity: Measures with detailed rules or timing are tougher.
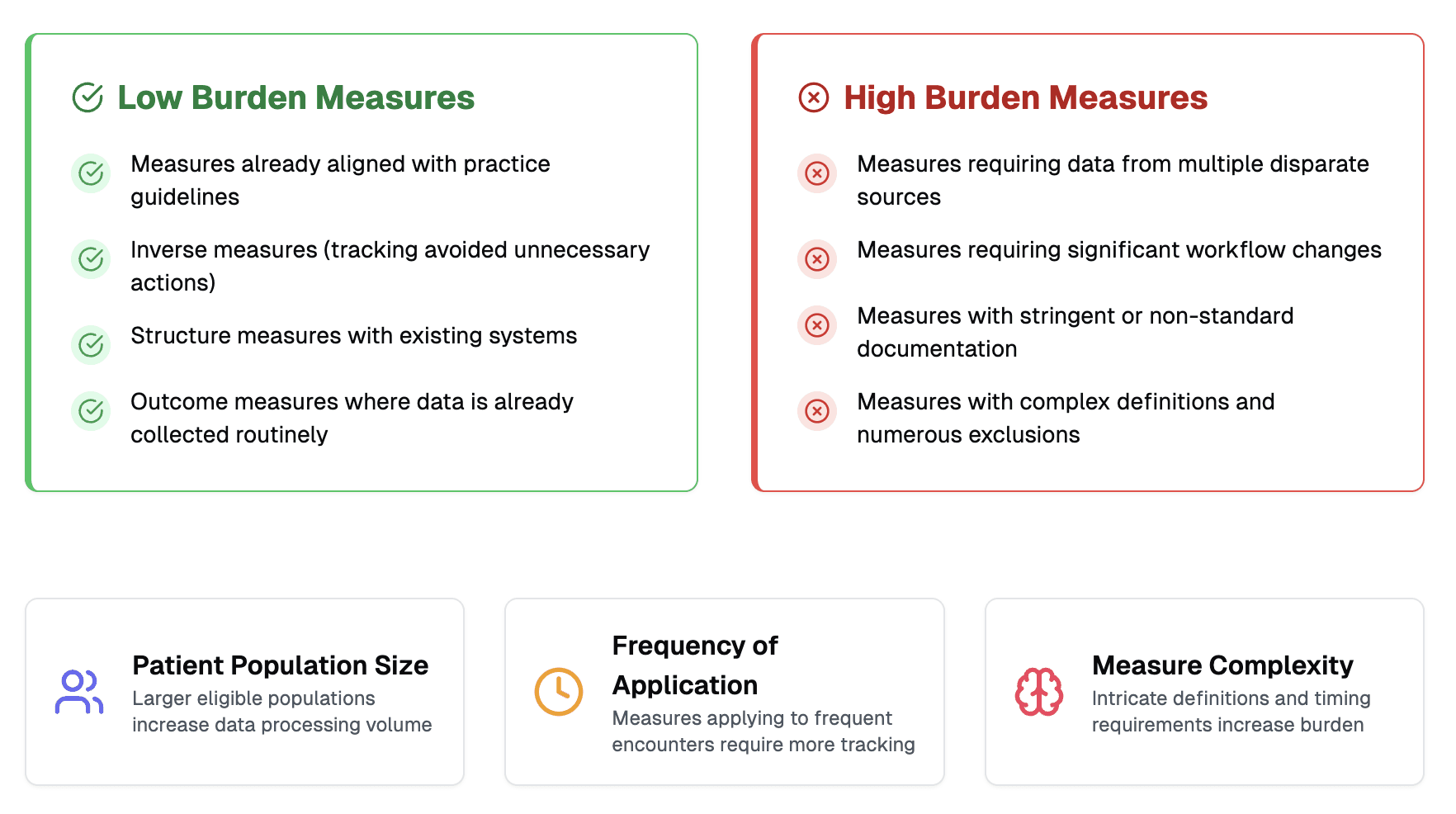
Some measures are low-burden, like those aligned with guidelines, inverse measures (e.g., avoiding unnecessary tests), or outcome measures if you already collect the data. Evaluate burden to ensure feasibility.
Examining the Documentation Requirements for MIPS Quality Measures
Documentation is a key part of measure burden. Measures often require specific notes, codes, or data fields to meet criteria. For example:
Counseling measures may need details on topic, time, and patient response.
Shared decision-making measures require notes on alternatives, risks, and preferences.
Claims reporting needs CPT II or G-codes on bills.
Documentation varies by submission method:
Claims: Needs specific codes, with lighter note-taking but strict coding.
EHR (eCQMs): Requires structured data in specific fields, which can disrupt workflows if misaligned.
Registry/QCDR: More flexible, pulling from broader data sources, easing clinician burden.
Precise documentation ensures cases count. Use templates or training to stay consistent.
The Role of a Measure Steward for MIPS Quality Measures
A measure steward is an organization—like a medical society, quality group, or CMS—that develops, maintains, and updates a MIPS Quality Measure. Stewards ensure measures reflect current clinical evidence, handling:
Writing clear specifications (denominator, numerator, etc.).
Testing measures for accuracy and feasibility.
Updating measures based on new evidence or feedback.
Providing guidance via FAQs or guides.
Knowing the steward can boost confidence in a measure’s relevance.
The Evidence Base Used by Measure Stewards to Create MIPS Quality Measures
Stewards base measures on strong evidence, including:
Clinical Guidelines: Expert recommendations from medical groups.
Research: Peer-reviewed studies, like trials or reviews.
Expert Consensus: Clinician agreement when evidence is limited.
Performance Data: Past MIPS data to assess feasibility.
Stakeholder Input: Feedback from providers and patients.
Measure specs cite this evidence, showing why the measure matters for quality care.
Categorizing MIPS Quality Measures: Understanding the Different Types
MIPS Quality Measures are grouped by focus:
Process Measures: Did you perform a recommended action? (e.g., ordering a screening)
Outcome Measures: Did care improve health? (e.g., controlled blood pressure)
Intermediate Outcome Measures: Short-term results (e.g., A1c levels)
Patient-Reported Outcome Measures (PROMs): Patient feedback on pain or function.
Efficiency Measures: Avoiding wasteful care (e.g., unnecessary imaging)
Structure Measures: Systems in place (e.g., EHR reminders)
Patient Engagement/Experience Measures: Satisfaction or communication feedback.
Outcome and high-priority measures carry more weight, so prioritize them.
How Are MIPS Quality Measures Scored?
The Quality category is typically 30% of your MIPS score. Your score comes from:
Performance Rate: Numerator ÷ Denominator × 100, compared to benchmarks.
Data Completeness: Report 75% of cases for full points.
Case Minimum: 20+ cases per measure.
Topped-Out Measures: May cap at 7 points.
Measure Type: Outcome/high-priority measures add points.
Bonuses: For electronic reporting or extra measures.
Your Quality score (up to 100 points) combines measure points and bonuses, impacting your Medicare payments.
How to Strategically Choose the Right MIPS Quality Measures
Picking the best measures maximizes your score:
Confirm Eligibility: Individual or group reporting?
Choose a Method: EHR, Registry, etc., to know available measures.
Match Your Practice: Pick measures for your patients and services.
Prioritize High-Value: Focus on outcome or high-priority measures.
Check Data: Ensure you can capture needed data easily.
Review Past Scores: Build on strengths from prior years.
Study Benchmarks: Understand national performance levels.
Report Six+: Include at least one outcome/high-priority measure.
Strategic choices align reporting with your quality goals.
Addressing Common Challenges in Reporting MIPS Quality Measures
MIPS reporting can be tough:
Data Issues: Inconsistent or hard-to-pull data.
Complex Specs: Detailed denominator or exclusion rules.
Completeness: Tracking 75% of cases all year.
Annual Updates: New measures or rules each year.
Workflow: Adding data capture steps.
Measure Choice: Picking relevant, high-scoring measures.
Tech Issues: Submission portal glitches.
Tracking: Monitoring performance in real-time.
Clear processes and tech partners help tackle these.
How Can Actuvi Help with MIPS Quality Reporting?
Navigating MIPS Quality reporting doesn’t have to be a burden. Actuvi offers solutions to simplify and optimize your MIPS process, letting you focus on patient care. Our expertise and technology help you:
Ensure Data Completeness: We capture data from EHRs, software, devices, and health apps to meet completeness requirements.
Incorporate Patient-Reported Data: Our app collects Patient-Reported Outcome Measures (PROMs) and Experience Measures (PREMs), capturing patient perspectives for key measures.
Integrate with Workflow: We fit into your clinical routines, making data capture efficient without disrupting care.
Streamline Data Management: We extract, validate, and aggregate data for CMS submission, reducing errors.
Partnering with Actuvi gives you the tools and expertise to approach MIPS confidently, maximizing your score and minimizing administrative burden while supporting quality care.
Putting It All Together
Successfully navigating MIPS Quality Measures is vital for optimizing your MIPS score, securing Medicare payments, and showcasing your dedication to exceptional care. This guide provides a detailed look at measures, from their definition and types to calculating denominators and numerators, scoring factors, and common challenges. By leveraging this knowledge, you can make informed decisions about measure selection and reporting.
Actuvi is here to help. Our technology simplifies the process, ensuring data completeness, capturing patient-reported data via our app, and integrating with your workflow. We help you maximize your MIPS Quality score and demonstrate the value of your care.
Don’t let MIPS reporting be a source of stress or missed opportunities. Contact Actuvi for a personalized consultation to streamline your reporting, overcome challenges, and achieve your MIPS goals while supporting continuous quality improvement.